Trigeminal neuralgia (TN) also called tic douloureux is characterized by intermittent, sharpshooting, lancinating pain occurring over the face.
It affects adults, usually over 50 years of age, with a slight female preponderance. There are no known predisposing factors and onset is usually spontaneous. Patients suffer from an electric shock-like sensation over the face, usually unilateral, which may involve the entire one half of the face or parts like around the eye, forehead region, over the cheek area, angle of mouth or/ and the lower jaw. They are stereotypical for the patient. The pain is spontaneous in onset and many times it comes when one brushes the teeth, swallows food, talks, touches certain areas over the face ( trigger points) or when exposed to a waft of cold air. There are periods of complete freedom from pain.
The pain occurs in clusters lasting for months to years and may be followed by remissions which can be months to years long. Cold weather is known to exacerbate the condition. It is not uncommon for patients to have had several, if not at least one of their teeth removed prior to neurology/neurosurgery consultation, as the cause of the pain may have been considered as tooth cavities.
The trigeminal nerve receives sensory information from the face. TN occurs due to the abnormal firing of electrical impulses from this nerve. The cause of this may be idiopathic or secondary to some structural lesion. In idiopathic cases, there will be usually an arterial, less likely a vein that touches the nerve as it enters the brainstem and deforms it resulting in abnormal nerve functioning. Idiopathic causes account for the most common etiology for TN(85%).
Secondary causes (15%) include lesions like epidermoids, meningiomas which grow in close proximity and press the trigeminal nerve. It is also important to rule out certain conditions like multiple sclerosis especially when the pain is bilateral and when it occurs in young individuals. Seek medical help from the best neurology hospital in Bangalore for Trigeminal Neuralgia Treatment
On examination by a neurosurgeon, the patients with idiopathic TN, do not have any neurologic deficits.
Diagnosis is based on mainly on clinical symptoms and findings, shored up by brain imaging with MRI. Special sequences in MRI known as T2 weighted and CISS 3D images are done to demonstrate the nerve conflict with a blood vessel. Imaging also identifies the presence of any other lesions or demyelination.
Once a diagnosis of TN has been made by the neurosurgeon, the first line of treatment includes medical management. The drug of choice is carbamazepine (CBZ). It is a given to stabilize the nerve’s electrical excitability. Invariably patients with TN have relief with CBZ. It is almost axiomatic that “ if a patient has relief with CBZ then the condition is TN else it is not”.
Unfortunately, after several months/years, the effectiveness of this drug wanes in many patients and they do not experience any relief with medication. A worrying problem of this wonder drug is its associated side effects which result in discontinuation of the medication in more than a quarter of patients. The side effects include drowsiness, giddiness, instability, double vision, low blood counts and allergic reactions. Other drugs used in TN though not as effective as the former are lamotrigine, baclofen, phenytoin, pregabalin, oxcarbazepine, though they may have lesser side effects.
If a patient benefits from medical management, it is continued for long durations even for several years. As TN has periods of remissions, patients are encouraged to try to reduce the drug doses and even stop if they are in remission period. Up to 25-50% of patients eventually stop responding to drug therapy and require some form of alternative treatment. Once medical management fails then the neurosurgeon considers surgical modes of management. The surgical procedures include certain percutaneous techniques, microvascular decompression of the nerve, and gamma knife radiosurgery.
Percutaneous procedures:
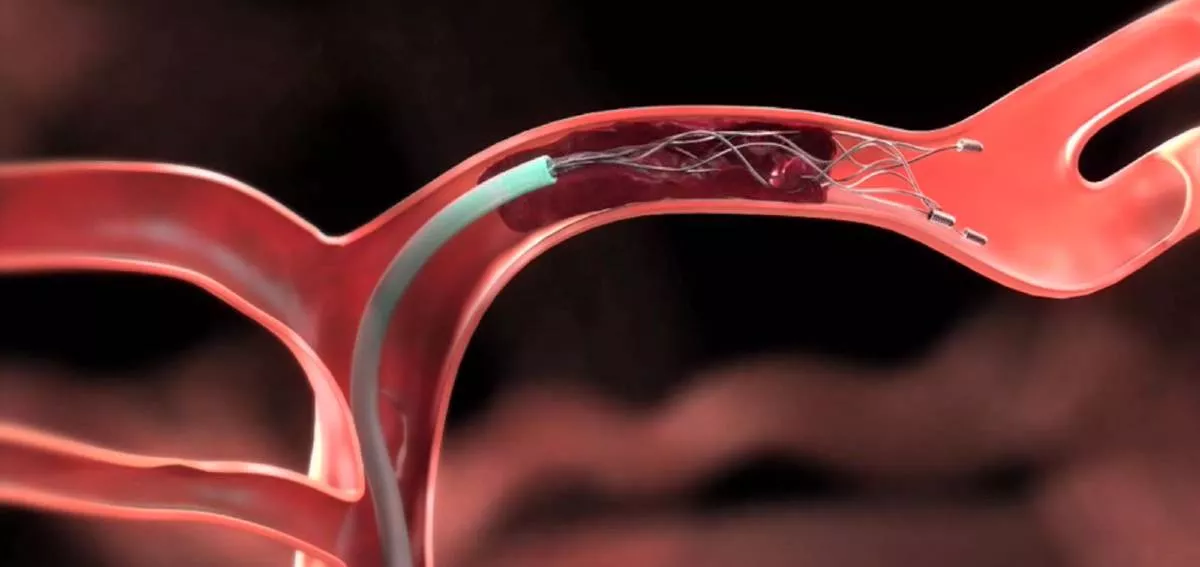
Percutaneous radiofrequency ablation of the trigeminal ganglion. In this procedure a needle is inserted into the base of the skull from the cheek region and a small current is delivered to the trigeminal ganglion. This results in relief of pain in 80-90 % of patients immediately. But the complications of anaesthesia with pain over various regions of the face (Anaesthesia Dolorosa) can occur. Recurrence of pain is seen in 3-4 years in many patients. This procedure cannot be done if there is pain around the eye region and forehead as anaesthesia over the eye can lead to disastrous eye damage.
Other percutaneous procedures include glycerol injection into the ganglia or balloon dilatation and comp[ression of the ganglion. Both are not very attractive, due to short pain-free intervals of 1-2 years and a relatively higher risk of complications.
Gamma knife radiosurgery: In this procedure, a frame is fixed on the head, an MRI is done and then a high dose of focused gamma radiation is delivered to the nerve. This results in a slow stabilization of the nerve. Though it is associated with a very low complication risk, its effectiveness is nothing to boast about. Immediate relief occurs after a month or so and in only about 50-60 % of cases. The long term recurrence rate is also high, with only 30-40% of cases having long term relief of pain. Hence this treatment modality is reserved for elderly, infirm patients, and those with high risk for surgery.
Microvascular decompression
Till date, this is the most effective treatment available. The immediate relief rates are as high as 98% and long-term recurrence chances are thereafter 10 to 15 years in a small subset of patients. In this procedure, the neurosurgeon opens the skull behind the ear and with precision reaches the trigeminal nerve. The blood vessel compressing the nerve is identified and very assiduously the tenuous nerve is separated from the blood vessel and a synthetic barrier usually Teflon is placed between the two. Relief from pain is immediately realized by the patient after reversal from anesthesia.
People with TN need not be despondent and should not be worried that they may develop a stroke or cancer in the brain or they may die due to pain. Early, appropriate treatment by neurosurgeons will result in long term good outcome in these patients.
Get in touch with Aster RV hospital in JP Nagar to consult one of the best neurologists in Bangalore.