Patient Information:
- Age: 30 years
- Sex: Female
- Marital Status: Married, 1 child
- Obstetric History: Previous Lower Segment Caesarean Section (LSCS) 8 years ago, with the birth of a male child.
- Medical History: No significant medical history.
Clinical Presentation:
The patient, a 30-year-old female, presented at 18 weeks of gestation with an anterior wall uterine fibroid measuring approximately 4 x 4 cm. The fibroid was noted on routine ultrasound during the second trimester, and the patient was monitored closely. At the time of presentation, she reported no significant complaints but was aware of the presence of the fibroid, which was growing along with the pregnancy.
The patient had a history of one previous LSCS (caesarean delivery) 8 years ago and had an uneventful recovery from that surgery. Her current pregnancy had been progressing without complications until around the third trimester when she experienced mild abdominal discomfort.
Progression of Fibroid Growth:
As the pregnancy advanced, the fibroid also increased in size. By 36 weeks of gestation, the fibroid had grown significantly to a size of 9 x 8 x 6 cm, located in the anterior wall of the lower uterine segment. The fibroid was now causing some pressure symptoms on the adjacent uterine structures, and there were concerns about its potential impact on the delivery process.
Ultrasound at 36 weeks confirmed the fibroid's position in the anterior lower uterine segment, and the fetus was noted to be in a favorable cephalic position. The patient was informed about the risks associated with the fibroid, including possible bleeding, preterm delivery, and complications during delivery. Given the size and location of the fibroid, it was decided that the patient would undergo elective LSCS with myomectomy at 38 weeks of gestation.
Surgical Management:
The patient was scheduled for an elective LSCS with myomectomy at 38 weeks of gestation. The decision for surgery was based on the following factors:
- The size and location of the fibroid, which could interfere with a vaginal delivery.
- The patient’s previous caesarean section and the associated risk of uterine rupture during labor.
- Preoperative Management:
- Routine preoperative workup, including blood tests and an assessment of fetal well-being, was conducted.
- The patient was counseled about the surgical procedure, including the potential for increased blood loss due to the fibroid and the risk of additional complications.
- Intraoperative vasopressin was planned to help reduce blood loss during myomectomy.
- Surgical Procedure:
The patient underwent elective lower segment caesarean section (LSCS) followed by myomectomy and bilateral tubectomy.- Anesthesia: Spinal anesthesia was administered.
- Incision: A standard lower transverse incision was made in the lower segment of the uterus.
- Fetal Delivery: A full-term male baby weighing 3.1 kg was delivered without any complications. Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. uterine incision closed with vicryl No. 1 in two layers.
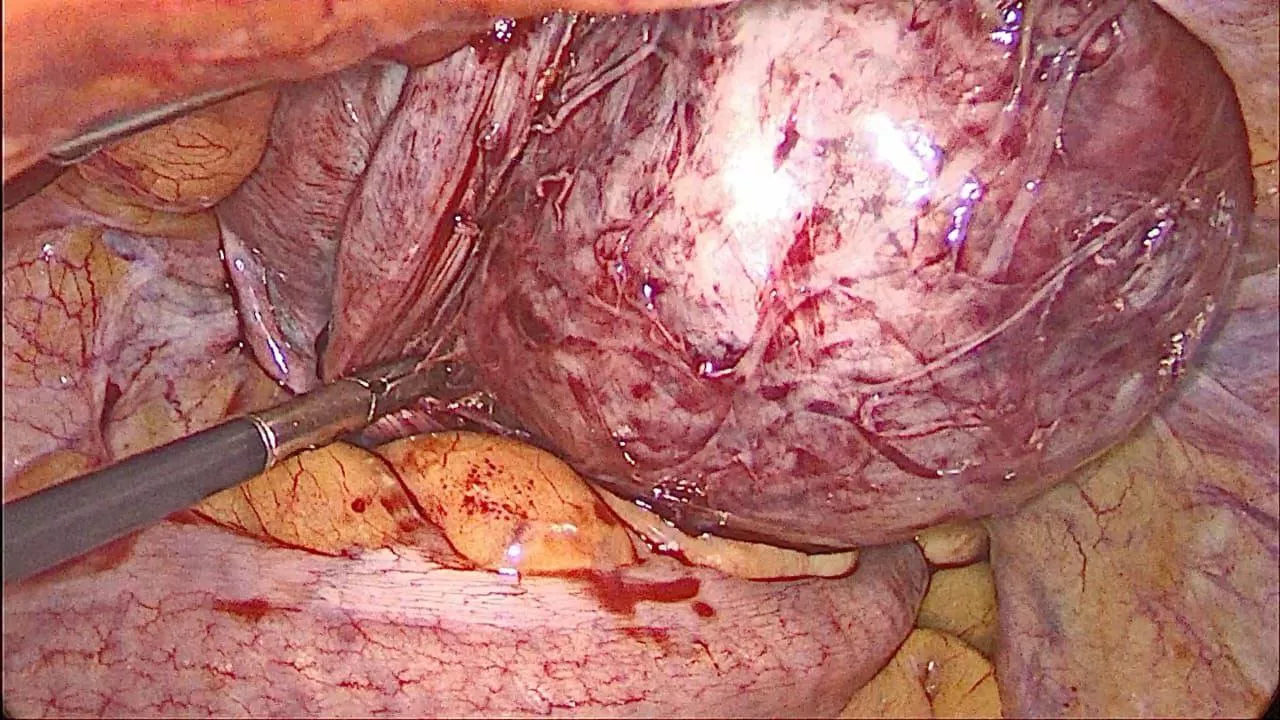
- Fibroid Enucleation: After fetal delivery, the large anterior wall fibroid (9 x 8 x 6 cm) was carefully enucleated from the lower uterine segment. The fibroid was located deep in the uterine wall, and careful dissection was required to avoid damage to the surrounding uterine tissue.
- Hemostasis: Diluted vasopressin (0.2 IU in 100 mL saline) was used to reduce blood loss. This allowed for adequate control of bleeding, especially around the fibroid bed, where vascularity was increased.
- Closure: The uterus was sutured in two layers using vicryl No. 1 sutures. hemostasis was thoroughly checked.
- Bilateral Tubectomy: Following myomectomy, a bilateral tubal ligation (tubectomy) was performed at the patient’s request for permanent sterilization. Abdominal Closure: The abdominal wall was closed in layers with vicryl and staples.
Postoperative Course:
- Postoperative Recovery: The patient recovered well from the surgery. She was monitored in the post-anesthesia care unit (PACU) for a few hours and was then transferred to the general ward.
- Blood Loss: Blood loss during surgery was estimated at 500 mL, which was within the expected range, thanks to the use of vasopressin.
- Pain Management: The patient was given analgesia through epidural catheter.
- Postoperative Care: She was started on a clear liquid diet and was able to resume normal oral intake on postoperative day 1.
- Urine Output: No issues were noted with kidney function, and the patient was observed for any signs of urinary tract complications, especially given her history of a previous caesarean section.
- Ambulation: The patient was encouraged to ambulate early, which helped reduce the risk of thromboembolic events.
The postoperative period was uneventful, and the patient was discharged on postoperative day 4 with advice on wound care, follow-up visits, and activity restrictions.
Outcome:
- Baby Outcome: The baby was healthy, male with a birth weight of 3.1 kg and no immediate complications. The neonate was transferred to the postnatal care unit for observation and was discharged home with the mother after a 48-hour stay.
- Maternal Outcome: The mother recovered well from both the caesarean section and the myomectomy. She was advised to avoid heavy lifting and strenuous activities for the next 6 weeks to allow for optimal uterine healing.
Discussion:
This case demonstrates the management of a pregnant woman with a fibroid in the anterior wall of the uterus, who underwent caesarean myomectomy at term. Uterine fibroids are common in pregnancy and can cause complications such as obstructed labor, increased blood loss, and abnormal fetal position. In this case, the fibroid was large enough to warrant surgical intervention. The decision to perform an elective caesarean section with myomectomy allowed for the safe delivery of the baby and removal of the fibroid without causing harm to the mother or fetus.
- Fibroids and Pregnancy: Fibroids can cause a variety of complications during pregnancy, including preterm labor, placental abruption, and fetal malpresentation. In this case, the location and size of the fibroid posed a significant risk for vaginal delivery, making a caesarean section the safest option.
- Myomectomy During Pregnancy: Although myomectomy is generally avoided during pregnancy due to the risk of preterm labor and complications, it was deemed necessary here to ensure a safe delivery. The careful use of vasopressin to control bleeding was effective in minimizing complications.
- Bilateral Tubectomy: The patient opted for permanent contraception via bilateral tubectomy, which was performed concurrently with the caesarean section. This is a common procedure for women who do not desire further pregnancies and wish to avoid the risks of additional surgeries.
Conclusion:
This case illustrates the successful management of a pregnant woman with a large anterior wall fibroid through a combined approach of LSCS, myomectomy, and tubectomy. By carefully managing the fibroid removal during a caesarean delivery, and using vasopressin to control blood loss, the surgical outcome was excellent, with both mother and baby doing well. This highlights the importance of individualized care for pregnant women with uterine fibroids, especially in terms of timing of surgery and minimizing risks to both mother and fetus.