
Ameloblastoma is a benign but locally aggressive odontogenic tumor that frequently necessitates radical resection to prevent recurrence. Reconstruction of mandibular defects, particularly those involving the condyle, remains challenging due to the need to restore both mandibular continuity and temporomandibular joint (TMJ) function. Virtual surgical planning (VSP) has emerged as an advanced technique enabling precise preoperative simulation, patient-specific implant design, and accurate intraoperative execution.
We present two cases of mandibular ameloblastoma managed with VSP-guided segmental mandibulectomy and immediate reconstruction using free fibula flaps. The first case, a 26-year-old female with involvement of the right mandibular ramus and condyle, required condylectomy and reconstruction with a patient-specific TMJ prosthesis integrated into the digital workflow. The second case, a 35-year-old male with disease confined to the right mandibular body, underwent fibula flap reconstruction alone. Both patients achieved satisfactory functional and aesthetic outcomes with no evidence of recurrence. These cases highlight the evolving role of VSP in enabling precise, predictable, and patient-specific mandibular reconstruction.
Introduction
Ameloblastoma accounts for approximately 1% of all oral tumors and is characterized by slow growth, local invasiveness, and a high recurrence rate if inadequately treated. Radical surgical excision with adequate margins remains the treatment of choice. However, reconstruction of mandibular defects is complex and requires restoration of facial symmetry, occlusion, mastication, and temporomandibular joint function.
The free fibula flap has become the gold standard for mandibular reconstruction due to its reliable vascular supply, adequate bone length, and versatility for multiple osteotomies. Nevertheless, conventional reconstruction techniques rely heavily on intraoperative judgment, which may result in variability in accuracy, prolonged operative time, and suboptimal contouring.
Virtual surgical planning (VSP) has evolved from stereolithographic modeling to advanced CAD-CAM–based workflows. It enables precise preoperative simulation of tumor resection, fabrication of patient-specific cutting guides, and production of customized reconstruction plates. In recent years, VSP has further expanded to integrate microvascular reconstruction with patient-specific temporomandibular joint prostheses, enabling complex hybrid reconstructions.
Importantly, the novelty of VSP lies in its ability to transform mandibular reconstruction from a surgeon-dependent, intraoperative approximation-based procedure into a fully pre-planned, digitally executed, and reproducible workflow. This paradigm shift allows direct translation of virtual three-dimensional planning into intraoperative accuracy, reduces variability, improves predictability of functional and aesthetic outcomes, and enables complex reconstructions that are difficult to achieve using conventional techniques.
CASE 1: Ameloblastoma involving right mandibular ramus and condyle
A 26-year-old female presented with an eight-month history of progressive swelling over the right mandible. Clinical examination revealed facial asymmetry with fullness over the right mandibular angle and ramus region, along with intraoral cortical expansion.
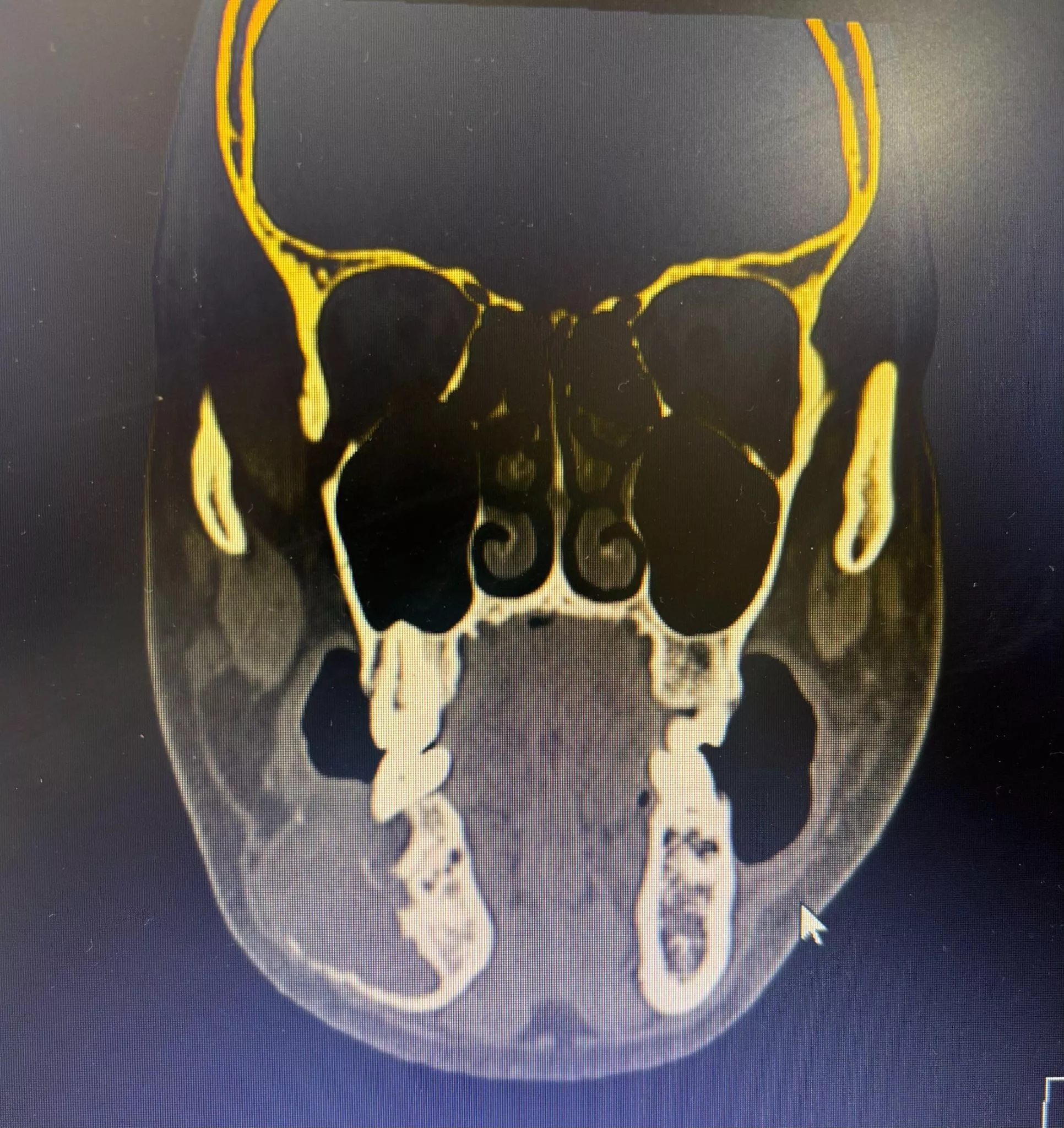
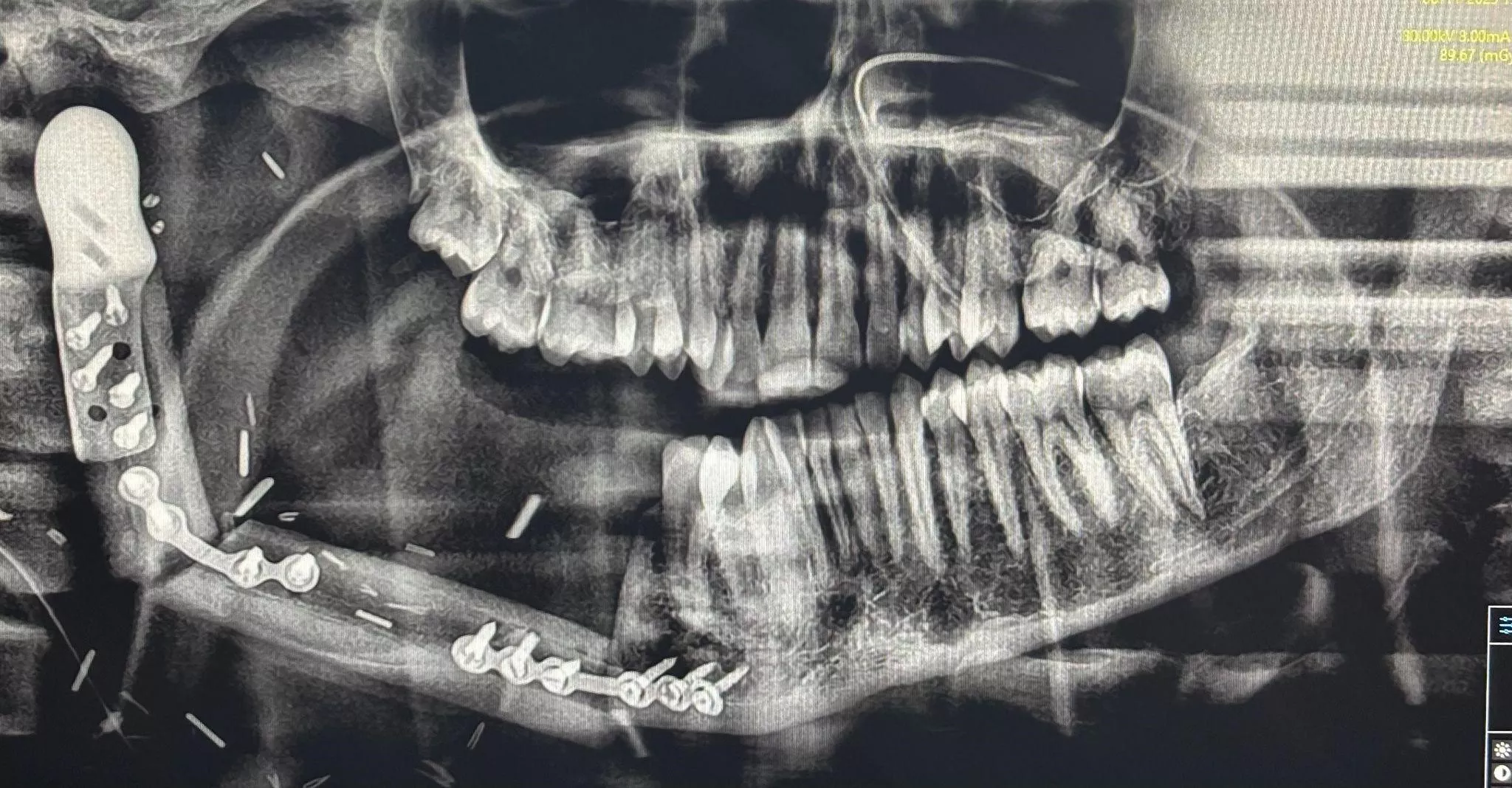
Orthopantomogram demonstrated a multilocular radiolucent lesion involving the right mandibular ramus extending into the condylar region. Computed tomography confirmed an expansile osteolytic lesion involving the right ramus and condyle. Histopathological examination confirmed ameloblastoma.
A right segmental mandibulectomy with condylectomy was planned, followed by immediate reconstruction using a free fibula flap and a patient-specific temporomandibular joint prosthesis.
Virtual surgical planning was performed using CT-based 3D reconstruction. Tumor margins were delineated with oncologic safety, and a simulated resection including the condyle was carried out. Fibula osteotomies were designed to restore mandibular contour, and a patient-specific TMJ prosthesis (fossa and condylar components) was fabricated along with cutting guides and a pre-bent reconstruction plate.
Surgery was performed according to the virtual plan. A right segmental mandibulectomy with condylectomy was completed using patient-specific guides. The TMJ prosthesis was positioned, followed by inset of the free fibula flap using pre-planned osteotomies. Fixation was achieved with a pre-bent reconstruction plate.
Postoperatively, the patient demonstrated stable temporomandibular joint function, satisfactory mouth opening, no deviation on opening, and good occlusion. Facial symmetry was well preserved.