
Large thoracic aortic aneurysms (TAA) are life-threatening conditions that can produce compressive symptoms on adjacent mediastinal structures — including the oesophagus, left atrium, and pulmonary veins. When patients present with dysphagia, dyspnoea, or chest pain driven by mass effect rather than rupture risk alone, timely intervention is essential.
Thoracic Endovascular Aortic Repair (TEVAR) has emerged as the preferred less-invasive alternative to open surgical repair, especially in elderly patients or those with significant surgical risk. Careful pre-procedural CT aortography and multidisciplinary planning are the cornerstones of a successful outcome.
Patient Overview
- 69-year-old male
-
Ex-smoker
-
Bilateral chest pain (1 month), dyspnoea on exertion, abdominal pain, and dysphagia for solids
-
No significant coronary artery disease; left ventricular function normal
Pre-Procedure CT Findings
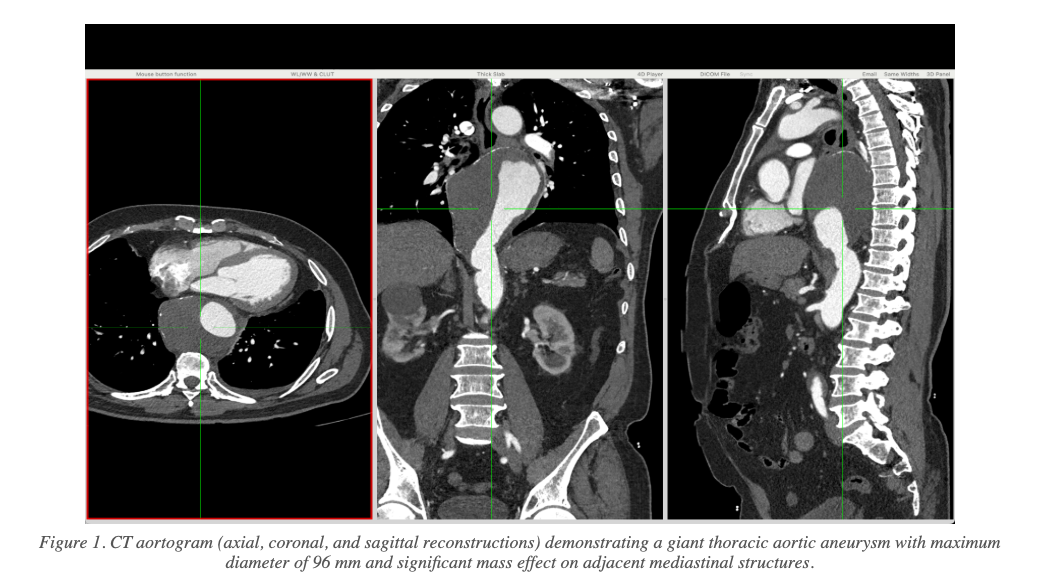
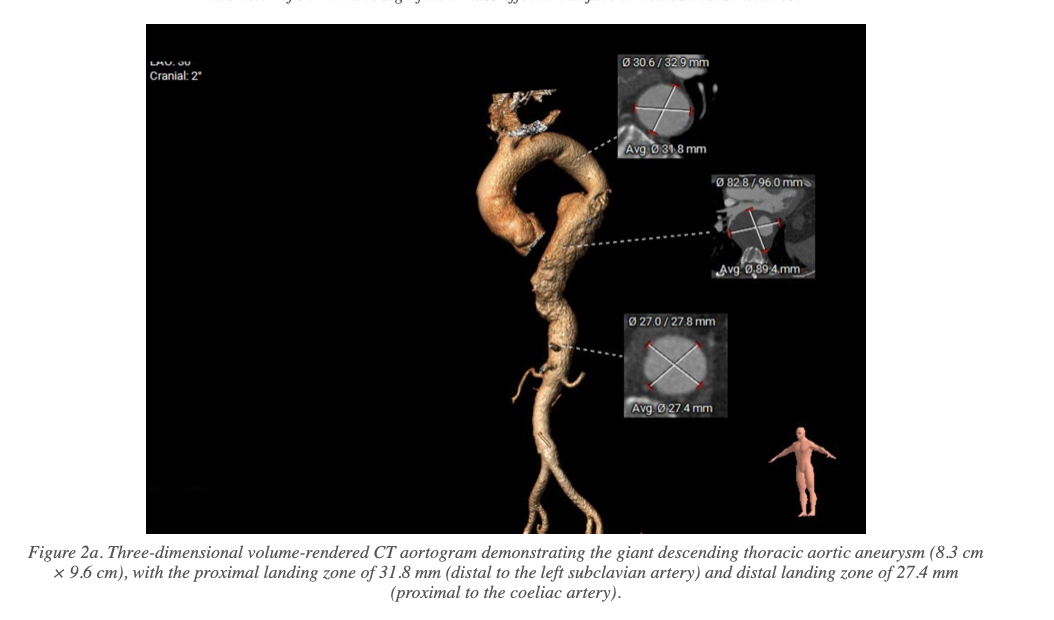
CT aortography revealed a giant descending thoracic aortic aneurysm with the following key measurements:
- Maximum aneurysm diameter: 8.3 cm × 9.6 cm
- Significant mass effect on the oesophagus, left atrium, and pulmonary veins
- Adequate proximal landing zone distal to the left subclavian artery (LSCA): 31.8 mm
- Adequate distal landing zone proximal to the coeliac artery: 27.4 mm
Intervention Strategy & Technical Approach
Following multidisciplinary review, the patient was taken up for elective TEVAR under general anaesthesia. The procedural steps were as follows:
- Right femoral artery (RFA) access via 20F sheath
- 5F left femoral artery (LFA) and left femoral vein (LFV) access for haemodynamic monitoring
- Lunderquist extra-stiff wire deployed for stable stent graft delivery
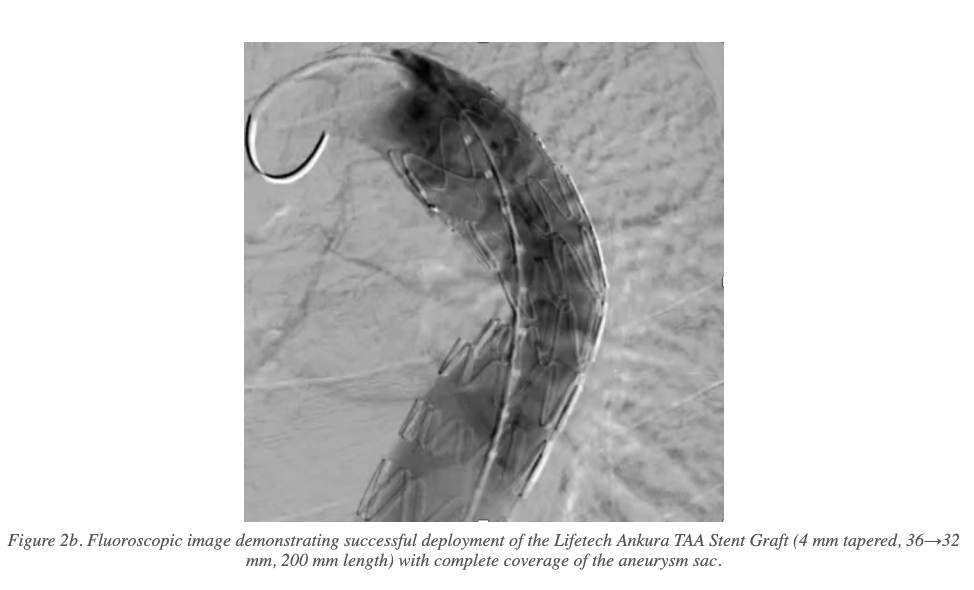
- Device: Lifetech Ankura TAA Stent Graft System — 4 mm tapered (36→32 mm), 200 mm length
- Post-dilation of the distal stent end performed with a Coda balloon to optimise apposition
- RFA access site closed with three Proglide sutures (percutaneous closure)
Follow-Up and Outcome
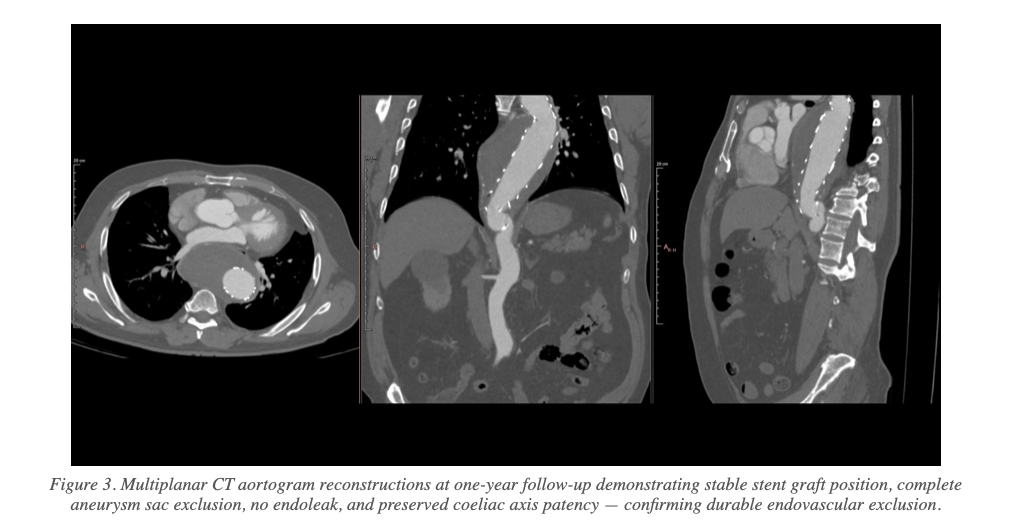
The patient had an uneventful post-procedural course. At clinical follow-up, he remained free of chest pain with significant resolution of compressive symptoms. One-year CT angiography confirmed:
- No endoleak detected
- No interval expansion of the aneurysm sac
- Stable stent graft position with good proximal and distal apposition at both landing zones
- Preserved patency of the coeliac axis
- Complete exclusion of the thoracic aortic aneurysm with satisfactory aortic remodelling
Conclusion
This case illustrates the effectiveness of TEVAR in achieving durable endovascular exclusion of a giant thoracic aortic aneurysm producing significant mediastinal compressive symptoms. The minimally invasive approach avoided the high morbidity associated with open surgery in this elderly patient.
Key takeaways:
- TEVAR is a safe and effective option for large TAA even in the setting of significant mass effect
- Precise pre-procedural CT planning is critical for appropriate device sizing and landing zone assessment
- Percutaneous access site management with Proglide sutures is feasible for large-bore access
- One-year imaging follow-up confirmed complete aneurysm exclusion with no adverse aortic events
References
1. Nienaber CA, Kische S, Rousseau H, et al. Endovascular repair of type B aortic dissection: long-term results of the INSTEAD trial. Circ Cardiovasc Interv. 2013;6(4):407–16.
2. Conrad MF, Tuchek J, Freezor R, Bavaria J, White R, Fairman R; VALOR II Investigators. Results of the VALOR II trial of the Medtronic Valiant Thoracic Stent Graft. J Vasc Surg. 2017 Aug;66(2):335–342.