
Case Summary
A 13-year-old girl presented with:
-
Intermittent high-grade fever for 1 week
-
Nausea and vomiting for 3 days
-
Swelling of hands and feet for 2 days
She had a history of exposure to SARS-CoV-2 one month prior, but remained asymptomatic at that time.
On admission, she was:
-
Febrile
-
Tachypneic and tachycardic
-
Hypotensive
-
Noted to have pulsus paradoxus
-
Elevated jugular venous pressure
-
Facial puffiness and peripheral edema
-
Decreased bilateral basal air entry
-
Distant heart sounds
Hepatomegaly was present, and the umbilicus was everted, suggesting fluid overload.
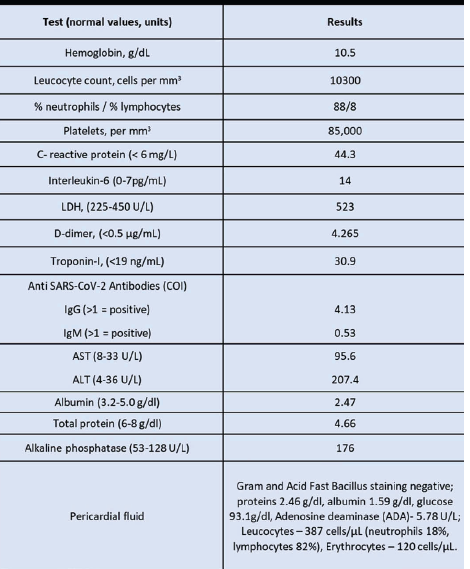
Her RT-PCR for SARS-CoV-2 was negative, but anti–SARS-CoV-2 IgG antibodies were positive, indicating prior exposure. Laboratory investigations revealed markedly elevated inflammatory markers.
Investigations
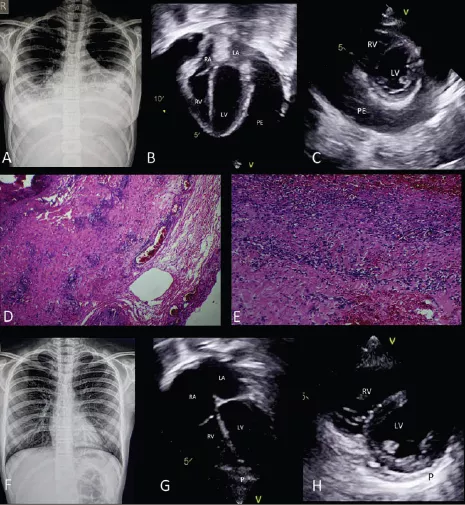
Chest Radiograph
-
Cardiomegaly (Fig 1)
-
Bilateral blunted costophrenic angles suggestive of pleural effusion (Fig 1)
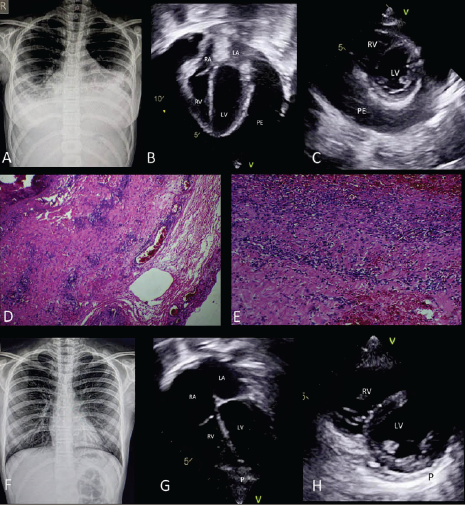
Echocardiography
-
Structurally normal heart
-
Massive pericardial effusion
-
Diastolic collapse of the right atrium and right ventricle
-
Normal biventricular systolic function
-
Bilateral pleural effusion
Findings were consistent with the physiology of cardiac tamponade.
Management
Given the presence of massive pericardial effusion with tamponade and bilateral pleural effusions, the patient underwent:
-
Emergency wide anterior pericardiectomy
-
Bilateral intercostal tube drainage
Approximately 650 mL of transudative pericardial fluid was drained.
Intraoperative findings:
-
Intense red discoloration of the epicardium and pericardium
-
Pericardial biopsy confirmed an acute inflammatory infiltrate
She was treated with:
-
Intravenous immunoglobulin (IVIG)
-
High-dose intravenous corticosteroids
Clinical and hemodynamic improvement occurred within 48 hours.
She was discharged after one week (following drain removal) on:
-
Tapering oral steroids
-
Aspirin
At 1-month follow-up:
-
She was asymptomatic
-
No residual pericardial effusion on echocardiography
Discussion
This case represents a rare and severe presentation of Multisystem Inflammatory Syndrome in Children (MIS-C) associated with prior Coronavirus disease 2019 (COVID-19) exposure.
While cardiovascular involvement is common in MIS-C, typical findings include:
-
Myocardial dysfunction
-
Coronary artery changes
-
Mild to moderate pericardial effusion
Severe pericardial effusion progressing to cardiac tamponade is exceedingly rare.
Pericardial involvement in acute COVID-19 is documented, but it is often associated with myocardial injury. In MIS-C, although pericardial effusion may occur, massive effusion requiring urgent surgical intervention has seldom been reported.
This case highlights:
-
The importance of recognizing pulsus paradoxus and tamponade physiology
-
The need for urgent echocardiographic evaluation in MIS-C patients presenting with shock
-
That shock in MIS-C can have multiple etiologies, including rare but life-threatening pericardial tamponade
-
The potential role of surgical intervention alongside immunomodulatory therapy