
60 year male, with multiple comorbidities like type 2 diabetes mellitus, hypertension, Poly-vascular disease; Chronic obstructive pulmonary disease (COPD), Chronic liver disease (CLD); Ischemic heart disease -Old Inferior wall myocardial infarction S/P PTCA + S RCA in (2015); Now presented with Acute coronary syndrome - Non-ST elevation Myocardial Infarction; LVEF 40%; with Cardio-renal Syndrome I over underlying chronic kidney disease.
Presented initially to outside hospital with complaints of chest discomfort, uneasiness and acute severe breathlessness. Was diagnosed to have NSTEMI with Pulmonary edema, stabilized with injectable diuretics and treatment for heart failure. Later was shifted to aster Aadhar hospital for further management.
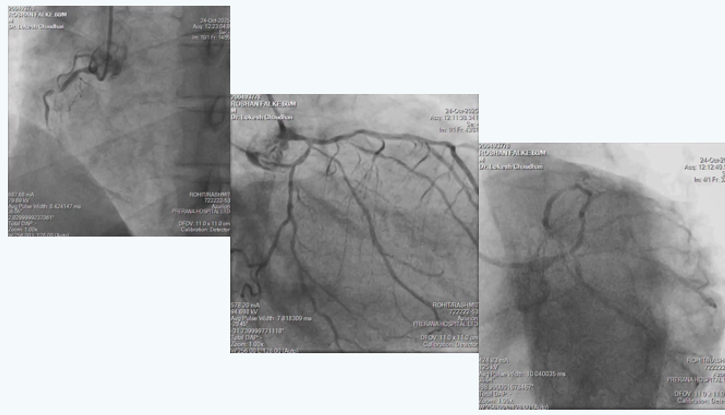
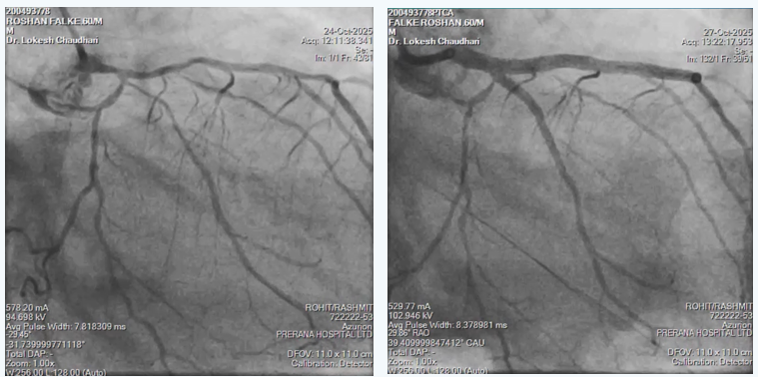
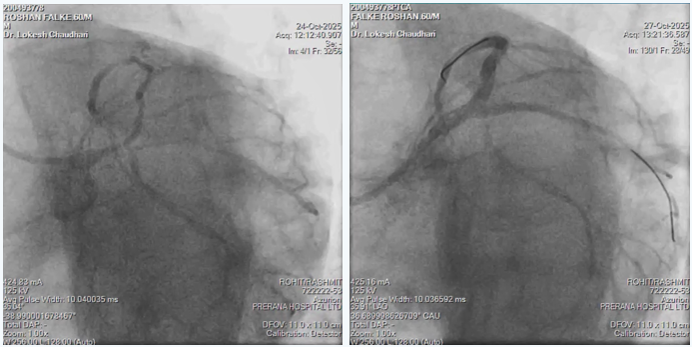
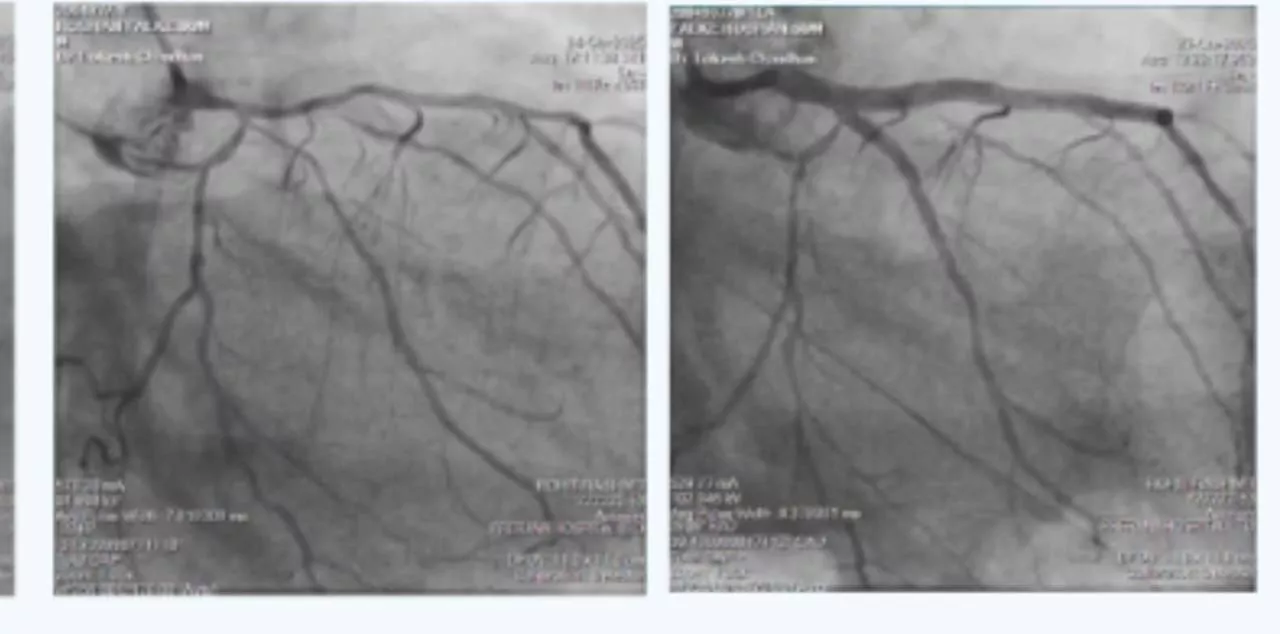
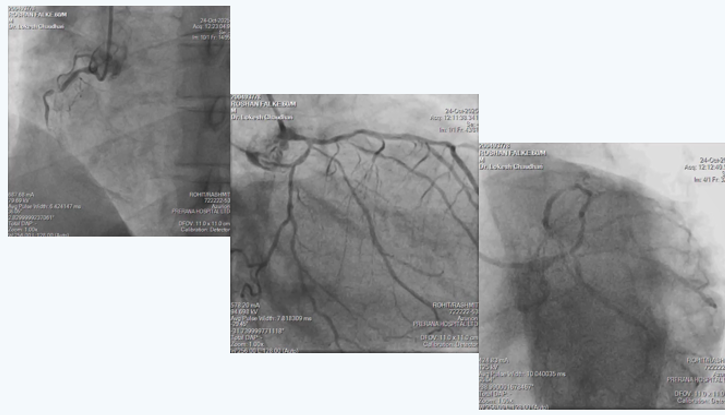
On arrival had mild dyspnea, no chest discomfort but had severe right lower limb pain since 6 hours, hence was started on heparin infusion and bilateral lower limb CT peripheral angiography was done which revealed Bilateral lower limb severe peripheral vascular disease with occlusion in bilateral femoral arteries and distal reformation through collaterals. Gradually patient was stabilized with heparin infusion alone. After 5 days, creatinine came to baseline of 1.5 and angiography wad done which showed Critical Left main with Triple vessel disease as shown in angiogram pictures. Patient had Right coronary artery in-stent-chronic total occlusion with filling of distal RCA from collaterals from LCA; Distal Left main had 80% narrowing with proximal LAD 70% and proximal LCX 80% stenosis.
In view of multiple comorbidities and patients preference, high risk complex multi-vessel PCI (Including RCA-ISR-CTO & LM-LAD-LCX bifurcation) was planned and done as per plan under local anesthesia from right radial artery access as CT aerogram showed diffuse peripheral vascular disease starting from abdominal aorta extending into bilateral femoral arteries.
Highlights:
- Complex multi-vessel disease done through 6F Radial access
- RCA-ISR-CTO opened using CTO techniques via 6F catheter
- LM-LAD-LCX bifurcation done using modified MINI-CRUSH technique through 6F catheter
- Entire procedure was done with 140 ml of visipaque without causing any worsening of renal function.