Severe Claudication: Total Aortoiliac Occlusion Managed with Modern Endovascular Technique
Introduction
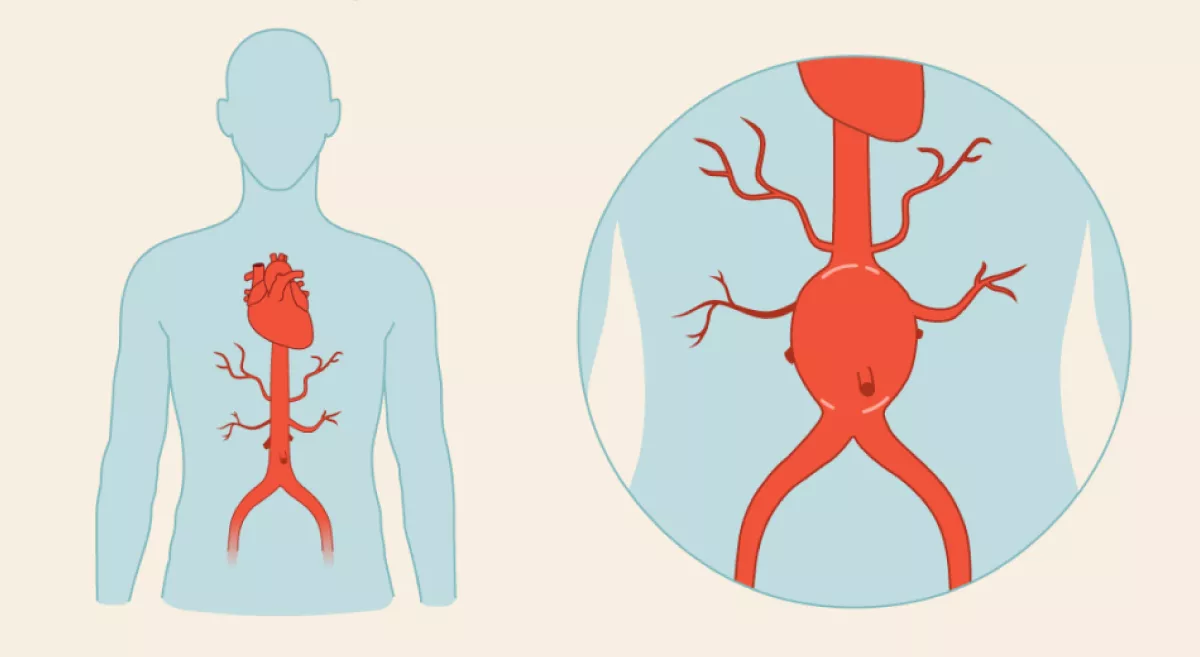
Aortoiliac occlusive disease is advanced peripheral arterial disease (PAD) involving infrarenal aorta and common iliac arteries, leading to critical limb ischemia and disabling claudication and tissue loss. PAD affects 3–10% of the population, rising to 15–20% after 70. Untreated, it can cause limb loss, reduced mobility, and increased cardiovascular mortality.
- Prevalence: PAD prevalence is 15–20% in those >70 years.
- Morbidity/Mortality: Untreated, 30% risk of resting pain/ tissue loss in 5 years; 20% 5-year cardiovascular mortality.
Case Summary
A 78-year-old man with ischemic heart disease, diabetes, hypertension, and severe disabling bilateral claudication could walk only 20–30 steps. Evaluation revealed total occlusion of the infrarenal aorta and bilateral common iliac arteries. Pedal pulses were absent. Considering comorbidities, open surgery was high risk. Instead, a complete endovascular reconstruction of aortic bifurcation (CERAB) was performed under local anesthesia using covered stents. The patient regained palpable pedal pulses and was discharged the next day.
Discussion Points
-
Endovascular techniques such as CERAB may avoid high-risk open surgery, even in frail, elderly patients.
-
Early diagnosis and referral prevent severe limb ischemia, which is often irreversible
What to look for in your practice
- Any patient >50 years with leg fatigue, cramps, or walking impairment should be screened for PAD- Ankle Brachial Index(ABI), Arterial Duplex ,CT/MR Angiogram.
- Assessment of peripheral pulses in lower limbs in at-risk populations.
Red Flag Symptoms
- Sudden decrease in walking distance
- Non-healing lower limb wounds or ulcers
- Rest pain in feet/toes
- Absent femoral/pedal pulses
When to refer to a vascular surgeon
Any patient with disabling claudication, rest pain, non-healing wounds, or absent pulses should be referred to a vascular surgeon.