
Chest wall neoplasms are a heterogeneous group of tumors that are challenging to both diagnose and treat. They can arise from any soft tissue or bony structure surrounding the thoracic cavity. These tumors may be primary or metastatic and may present as either symptomatic or asymptomatic lesions. Malignant rib tumors include multiple myeloma, chondrosarcoma, osteosarcoma, and Ewing’s sarcoma, which typically manifest as painful, rapidly growing, large palpable masses. Desmoid tumors and neurogenic tumors are benign but locally aggressive and rare tumors of the chest wall. Incorrect diagnosis, incomplete resection, and unsuccessful reconstruction of large thoracic wall defects have been associated with high rates of perioperative morbidity and mortality.
Chest wall resection and reconstruction is the primary surgical treatment for chest wall tumors. This procedure involves removal of one or more ribs to excise the tumor, followed by reconstruction to restore chest wall stability and achieve an acceptable cosmetic outcome. Reconstruction may involve the use of prosthetic materials and/or rotation of muscle flaps.
We present the case of a 70-year-old female who presented with a painless, hard swelling involving the left chest at the inner aspect of the left breast. The swelling gradually increased in size and later became mildly painful. Core biopsy was reported as a low-grade spindle cell tumor. Immunohistochemistry suggested low-grade spindle cell proliferation, probably mediastinal fibrosis. The spindle cells expressed SMA focally and were negative for desmin, CD34, beta-catenin, STAT-6, and S-100 protein.
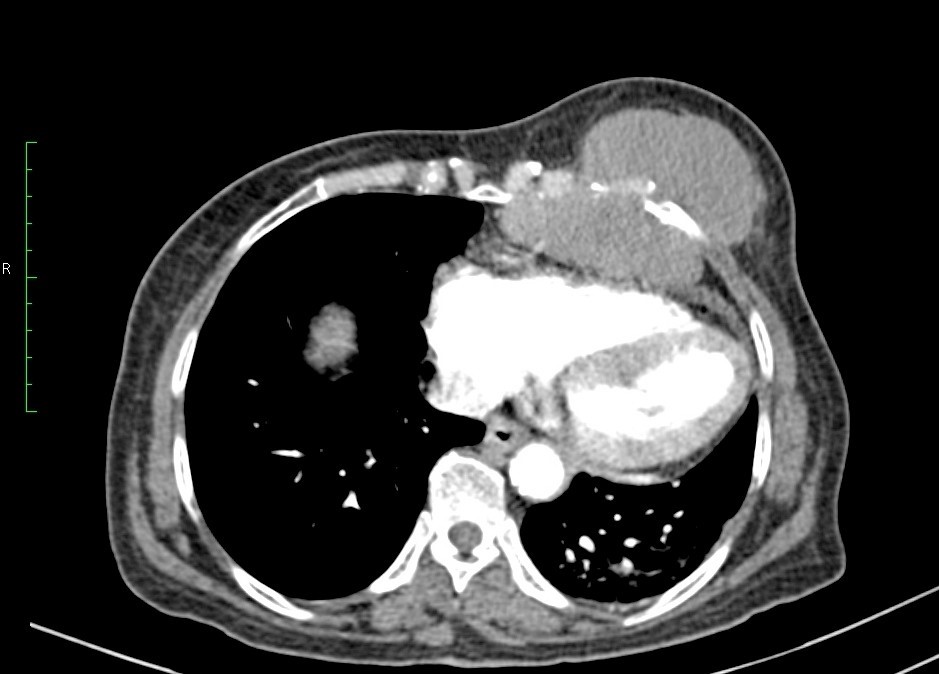
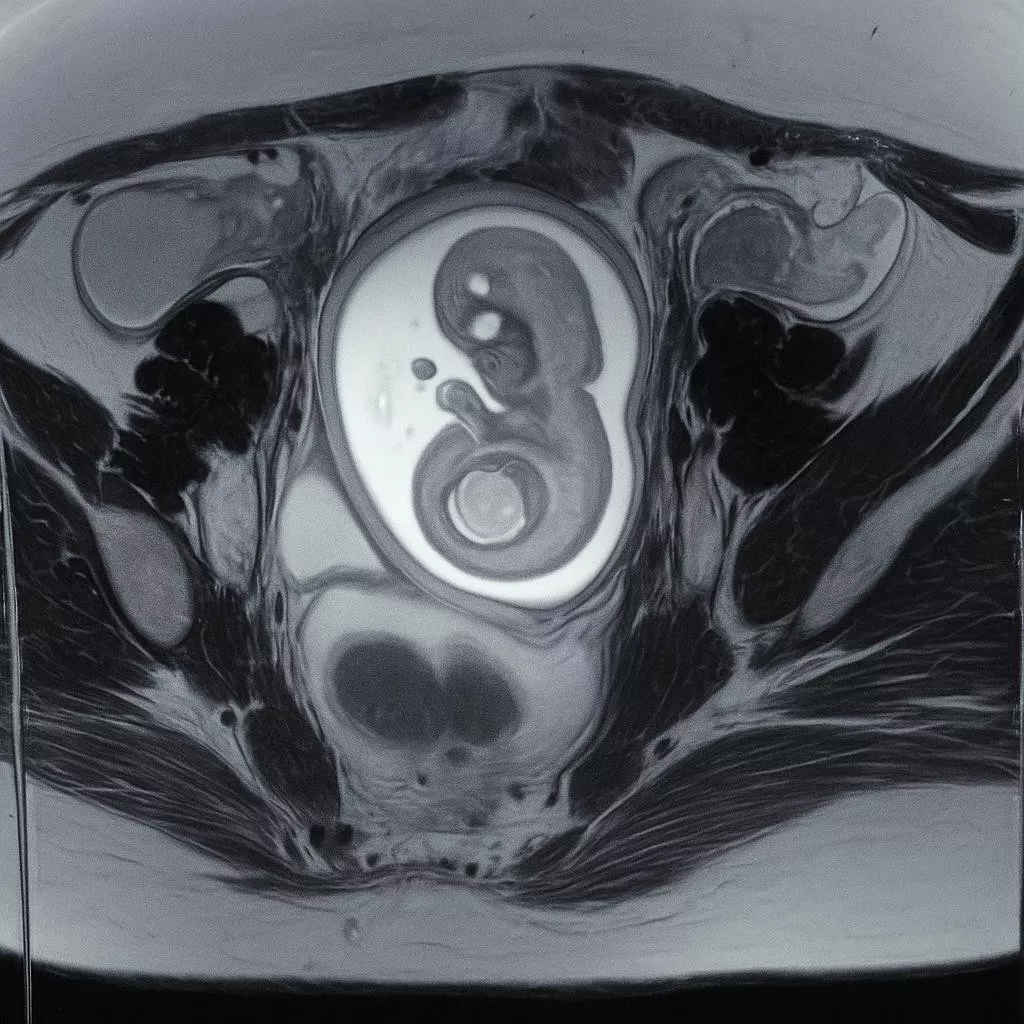
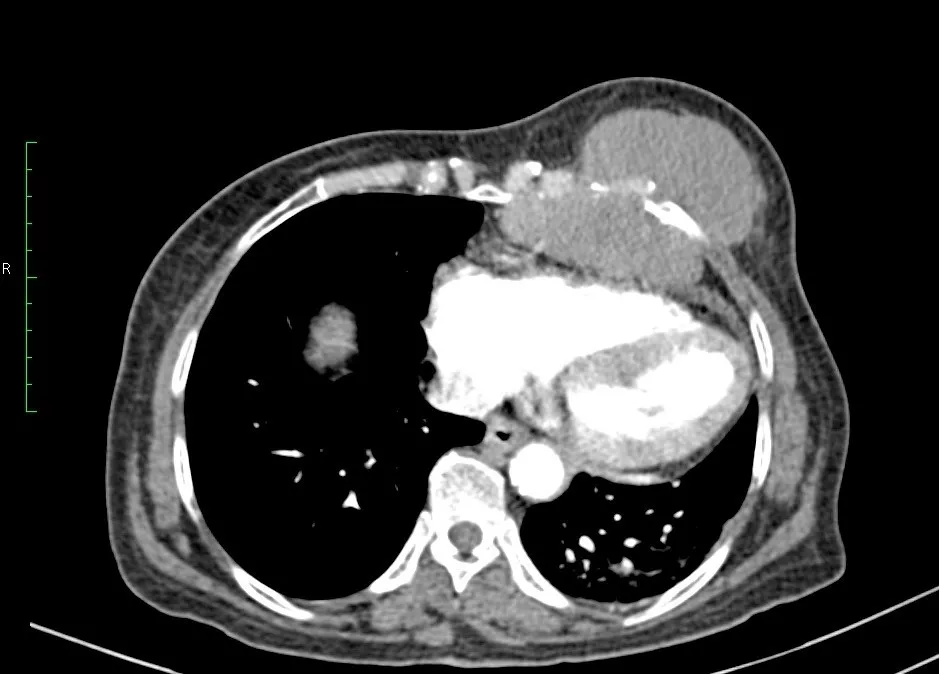
The patient defaulted on the advised surgery and presented again after 7–8 months with a significantly enlarged and painful swelling. Contrast-enhanced CT (CECT) of the thorax revealed a well-defined, heterogeneously enhancing lobulated soft tissue density lesion measuring approximately 10 × 9.3 × 7.1 cm. The lesion was epicentered in the left paramedian anterior aspect of the lower chest wall, causing erosion of the adjacent 4th to 6th ribs at the costochondral junction. An intrathoracic extrapleural component was noted, indenting the adjacent right atrium of the heart, with a distinct interface between the lesion and the pericardium. Adjacent lung volume loss was also observed. Anteriorly, the lesion extended up to the subcutaneous plane.
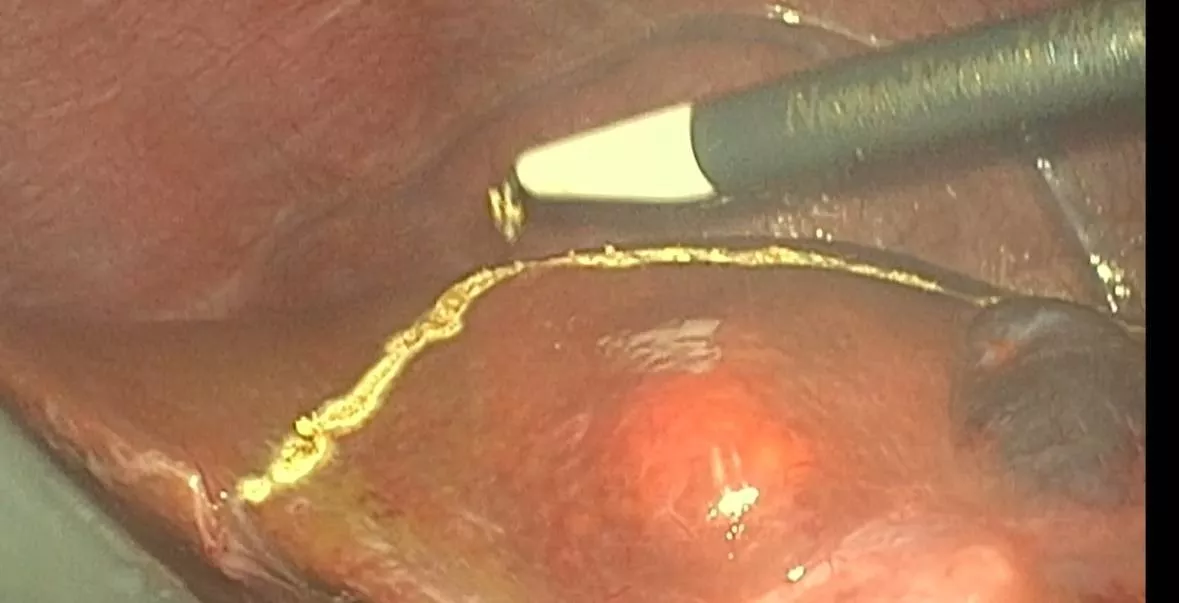
After pre-anesthetic evaluation, the patient underwent surgery. An incision was made along the left inframammary crease, and the breast was elevated to expose the tumor. Wide excision of the tumor was performed along with full-thickness resection of the 4th to 6th ribs and part of the serratus anterior muscle, ensuring adequate margins.
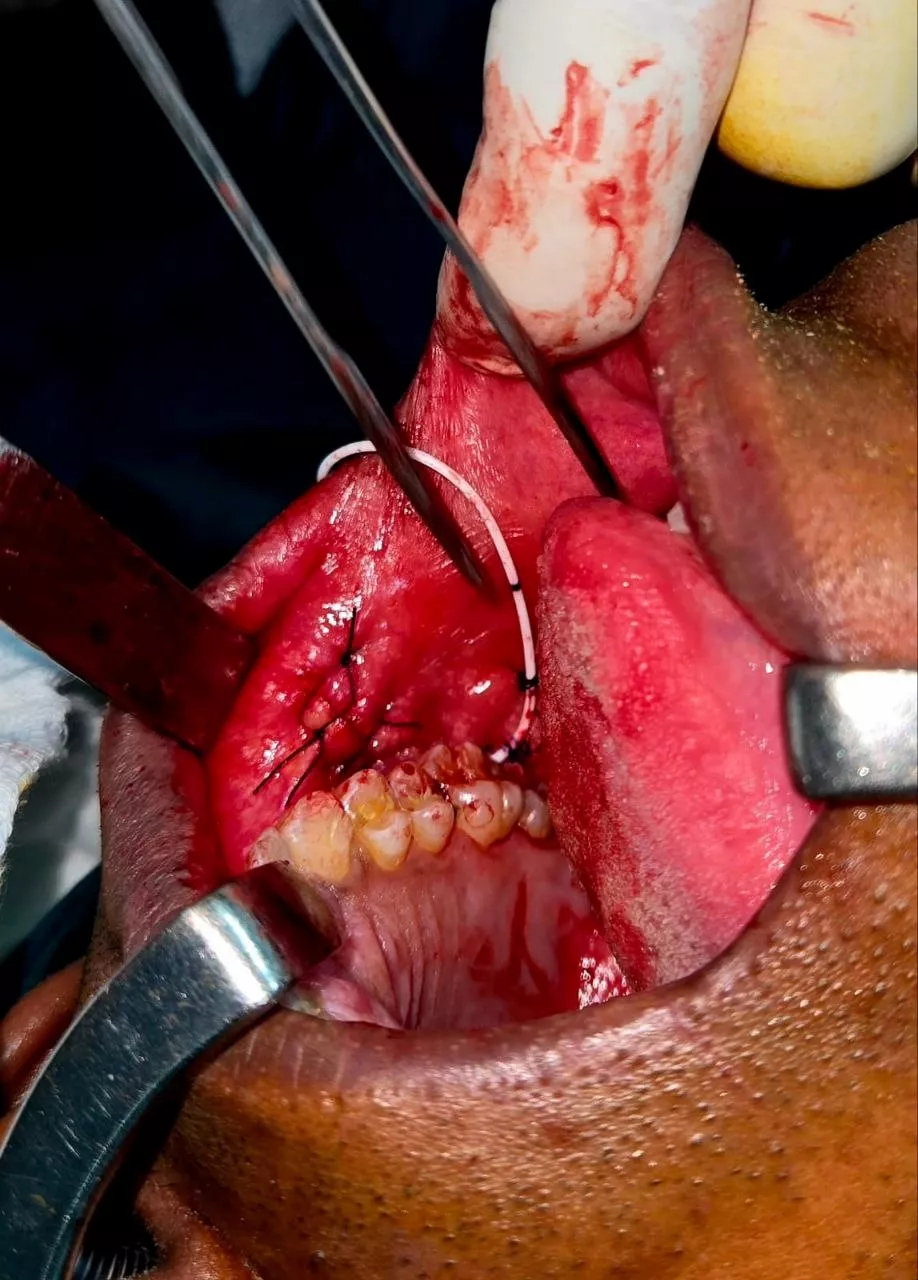
The resulting full-thickness chest wall defect was reconstructed using bone cement wrapped in Prolene mesh, which was secured to the cut margins of the resected ribs using No. 1 Prolene sutures. A pectoralis major myofascial flap was mobilized to reinforce the reconstructed area. A left intercostal drain was placed, and a suction drain was positioned at the reconstructed site beneath the pectoralis muscle.
The duration of surgery was 150 minutes, with a total blood loss of 150 mL. At our leading oncology hospital in India, the procedure was performed by experienced surgical oncologists in India, ensuring meticulous planning and precision. Final histopathology reported a low-grade spindle cell tumor with wide and adequate soft tissue and bony margins, microscopically free of tumor. The patient was discharged in stable condition on postoperative day 5, with all drains removed and no complications.