
Introduction
Adnexal masses are encountered in approximately 1 in 1,000–2,000 pregnancies. The majority are benign, with malignant or borderline ovarian tumors (BOTs) being exceptionally rare. BOTs account for ~15% of epithelial ovarian tumors and typically present in young women, making fertility preservation a key consideration.
Management during pregnancy presents unique challenges:
- Overlapping symptoms with pregnancy,
- Limited imaging options, and
- Dual responsibility of ensuring maternal oncologic safety and fetal survival.
Here, we report a rare case of bilateral serous borderline ovarian tumors in a 15-week primigravida, successfully managed with fertility- and pregnancy-preserving oncologic surgery.
Case Presentation
Patient: A 26-year-old primigravida (G1P1) presented at 15 weeks gestation with one month of abdominal pain.
Examination: General condition and vitals were normal. Abdominal examination revealed mild right-sided tenderness. Per vaginal examination was not performed.
Investigations:
- Early first trimester NT scan (11–13 weeks): Nuchal translucency 1.42 mm, nasal bone present, tricuspid/DV Doppler normal. Risk for trisomy 21, 18, and 13 negligible.
- Ultrasound (13–14 weeks): Live fetus, CRL 80.9 mm, FHR 168 bpm, no anomalies. Bilateral ovarian cysts noted (right ~69×51 mm, left ~32×24 mm) with papillary projections.
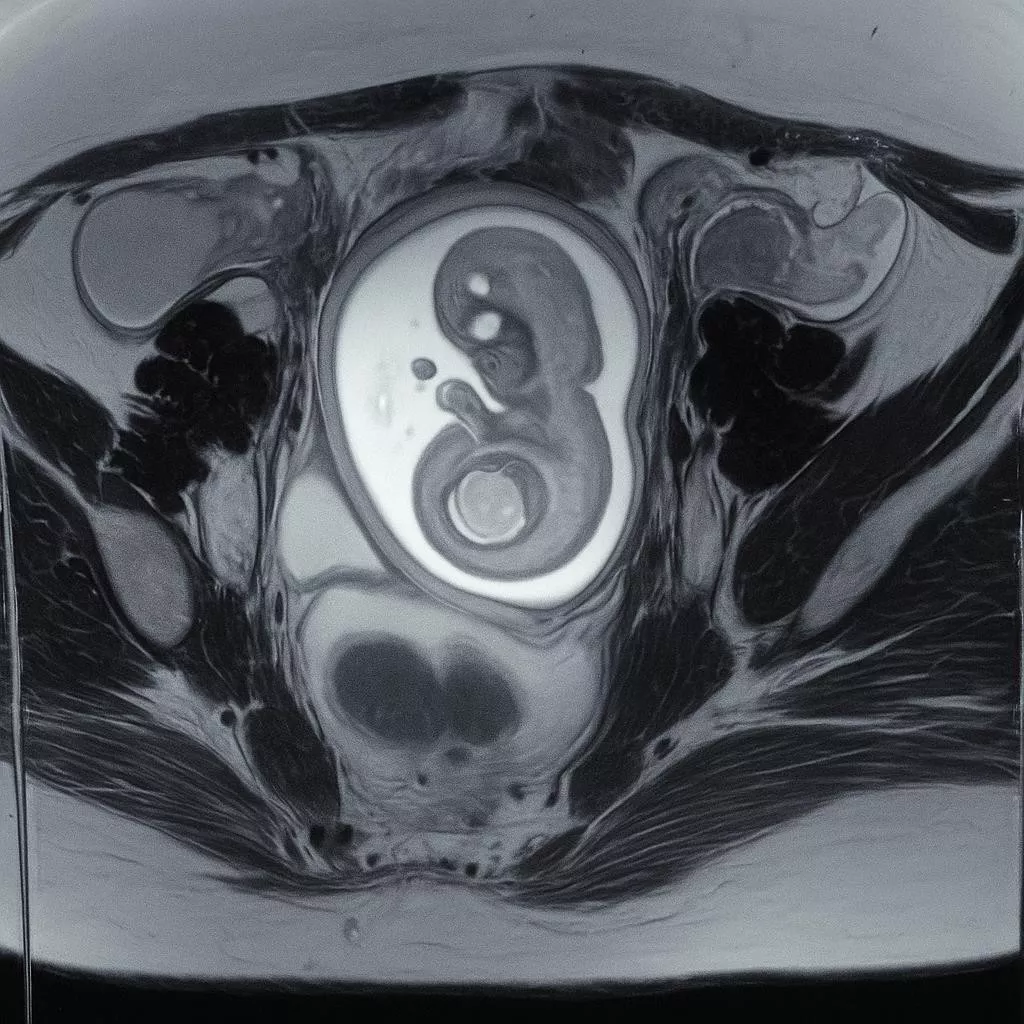
- MRI pelvis (12/07/2025): Right adnexal mass 75×55×46 mm, left adnexal mass 30× 25×53 mm, both complex with septations and vascular papillary projections; no extra-ovarian spread.
- Tumor markers: CA-125 >10,000 U/mL, CA19-9 = 400 U/mL.
- Fetal viability: Confirmed, no structural anomalies.
Pre-operative Planning: The case was discussed in the multidisciplinary tumor board. The plan was right salpingo-oophorectomy, left ovarian cystectomy vs salpingo-oophorectomy depending on frozen section, with complete staging. The patient and family were counselled regarding maternal–fetal risks and gave informed consent.
Surgical Management
- Approach: Midline laparotomy under general and epidural anesthesia.
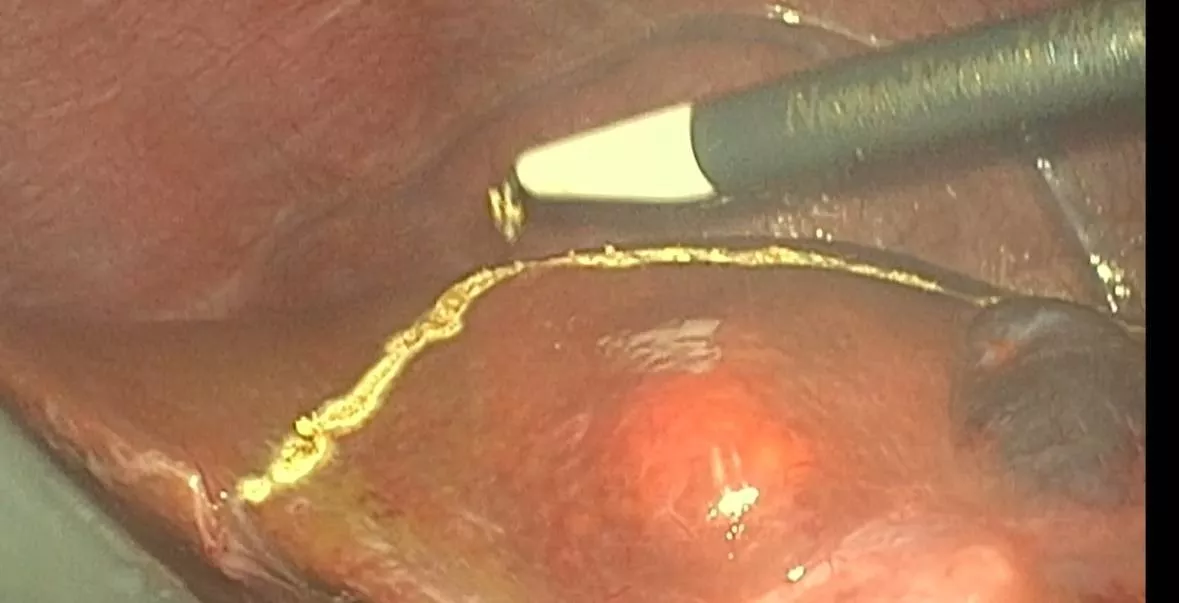
- Findings: Bilateral complex ovarian cysts; gravid uterus of 15 weeks; no ascites or peritoneal deposits.
- Procedure:
- Right ovary: capsule opened, spillage prevented and material sent for frozen section →
borderline serous tumor → right salpingo-oophorectomy performed.
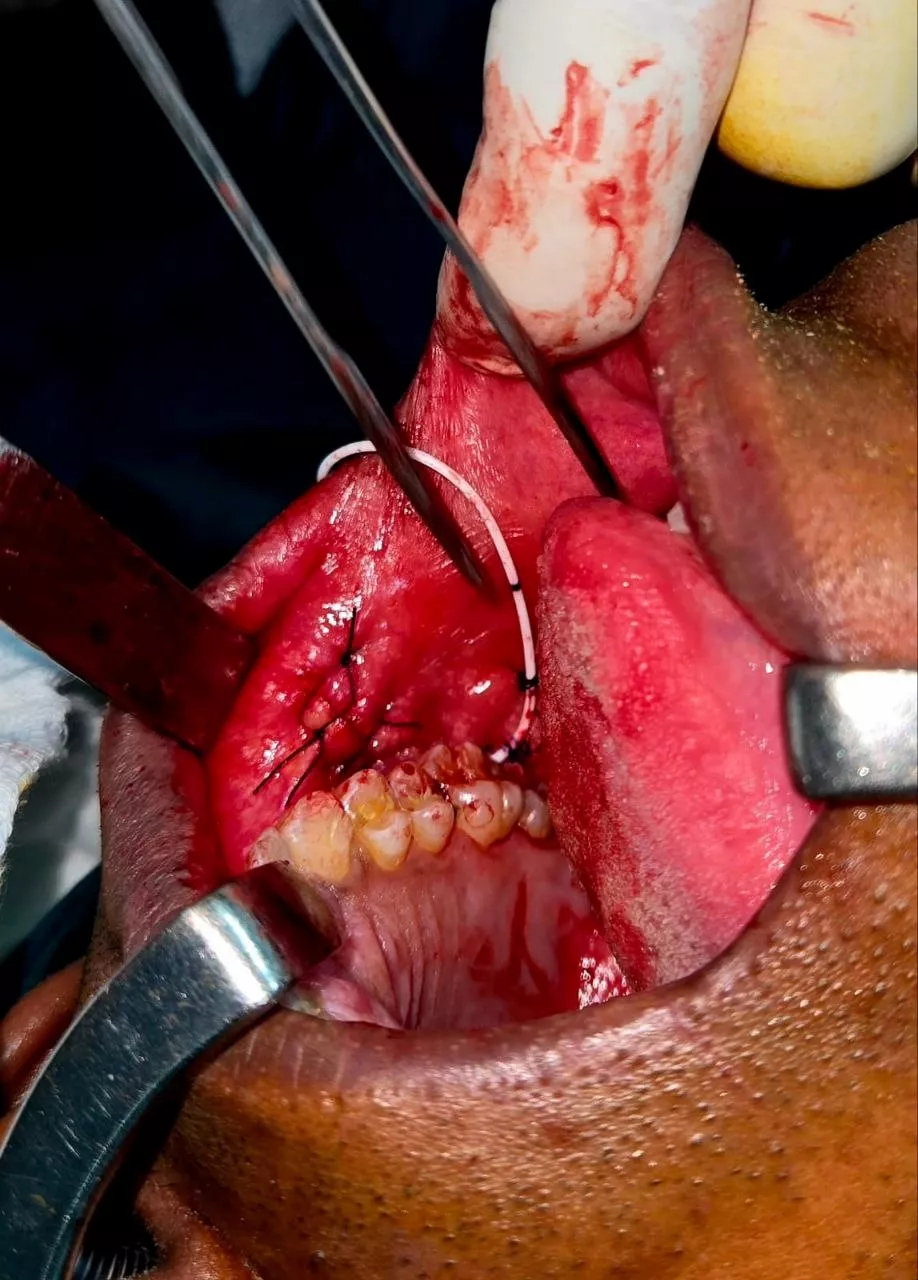
- Left ovary: lesion involving part of the ovary, intra-op ultrasound guided wide local excision; frozen margins negative → ovarian preservation with reconstruction using vicryl.
- Staging: Bilateral pelvic LN dissection (23 nodes), retroperitoneal LN dissection (7 nodes), infracolic omentectomy.
- Intra-op fetal monitoring: Continuous; fetal heart remained normal.
Histopathology
- Right ovary: Serous borderline tumor, capsule ruptured intra-op.
- Left ovary: Serous borderline tumor, margins negative.
- Nodes: Right pelvic 0/19, left pelvic 0/4, retroperitoneal 0/7 → all negative.
- Omentum: No deposits.
- Stage: FIGO Stage IC1 (capsule rupture).
- Final diagnosis: Bilateral serous borderline ovarian tumors, T1cN0M0.
Postoperative Course
- Maternal recovery was uneventful.
- Fetal viability confirmed by ultrasound during admission and at discharge.
- Patient was discharged on post-operative day 6 with a viable intrauterine pregnancy.
- Adjuvant chemotherapy was planned up to the third trimester, with obstetric follow-up.
Evidence-Based Discussion
Borderline ovarian tumors (BOTs) during pregnancy are extremely rare, occurring in fewer than 1 in 10,000 pregnancies. Most adnexal masses identified in pregnancy are benign, with malignancies accounting for less than 1% of cases, and bilateral BOTs are exceptionally uncommon. Early first- trimester screening, including nuchal translucency, ductus venosus, and tricuspid flow assessment, is important to reassure fetal well-being and exclude major chromosomal anomalies. For characterization of adnexal masses during pregnancy, MRI is preferred, as it can distinguish simple cysts from complex neoplasms, with papillary projections and septations suggesting BOTs. Tumor markers such as CA-125 can be physiologically elevated in early pregnancy, but levels above 200 U/mL, particularly in the presence of suspicious imaging, are concerning for malignancy. The second trimester, between 12 and 20 weeks, is considered the safest period for oncologic surgery, as it minimizes the risks of miscarriage and preterm labor. Surgical management emphasizes fertility-sparing approaches in reproductive-age women. Intraoperative frozen section aids decision-making, though it may misclassify tumors in about 20% of cases. Comprehensive staging—including salpingo-oophorectomy, peritoneal washings, omentectomy, and lymph node sampling—is recommended to confirm localized disease, as lymph node metastasis is rare but prognostically significant. Stage I BOTs have an excellent prognosis, with a five-year survival rate exceeding 95%. Fertility-sparing surgery may be associated with a higher recurrence risk of 20– 30%, but most recurrences remain borderline and are manageable surgically. Lifelong surveillance is therefore strongly advised.
Conclusion
Fertility-preserving oncologic surgery for bilateral borderline ovarian tumors can be performed safely in the second trimester, ensuring both maternal oncologic safety and fetal viability. Multidisciplinary decision-making and intra-operative frozen section are vital for tailoring management.
Patient Consent
Written informed consent was obtained from the patient for publication of clinical details and images. Identity has been protected.
Outcome: Final histopathology confirmed bilateral serous borderline ovarian tumors, FIGO Stage IC1 (due to intra-operative intentional capsule rupture, under controlled conditions). Omentum and >30 lymph nodes were negative. Maternal recovery was uneventful, and the fetus remained viable. As per histopathology report no adjuvant chemotherapy was advised.
Conclusion: This case illustrates the feasibility of fertility-sparing oncologic surgery in the second trimester for borderline ovarian tumors, with preservation of pregnancy. Multidisciplinary collaboration and intra-operative frozen section are critical in achieving dual goals of oncologic clearance and fetal safety.