Patient Details:
- Age/Sex: 36y/female
- Hospital: Aster Aadhar Hospital
- Consultant Surgeon: Dr. Nikhil Vinod Gulavani
- Date of Surgery: 25/08/2025
Case Summary:
The patient presented with multicentric triple-negative breast carcinoma (TNBC) of the left breast, with nodal and skeletal involvement. She received neoadjuvant chemoimmunotherapy achieving complete metabolic and pathological response. Definitive surgical management included robotic nipple- and skin-sparing mastectomy (R-NSSM) with DIEP flap whole-breast reconstruction.
Initial Evaluation:
- Histopathology: Invasive ductal carcinoma, Grade III, ER/PR/HER2 negative.
- Baseline PET-CT: Multicentric hypermetabolic lesions in left breast (SUVmax 16.0), hypermetabolic axillary, subpectoral, internal mammary, and supraclavicular nodes; FDG uptake in D9 vertebra (SUVmax 7.4).
- Diagnosis: Multicentric TNBC with nodal and skeletal involvement [oligometastatic].
Management Plan:
- Neoadjuvant Therapy: Pembrolizumab, Paclitaxel, Carboplatin, followed by Adriamycin + Cyclophosphamide + Pembrolizumab.
- Response Assessment: PET-CT showed complete metabolic response; no residual disease.
Treatment Plan:
Definitive surgery with robotic nipple- and skin-sparing mastectomy and DIEP flap reconstruction to achieve oncological clearance with optimal cosmetic outcome.
Procedure Performed:
- Approach: Robotic R-NSSM with DIEP flap reconstruction using SSI Mantra 3.0.
- Positioning: Supine, left arm abducted, under general anesthesia.
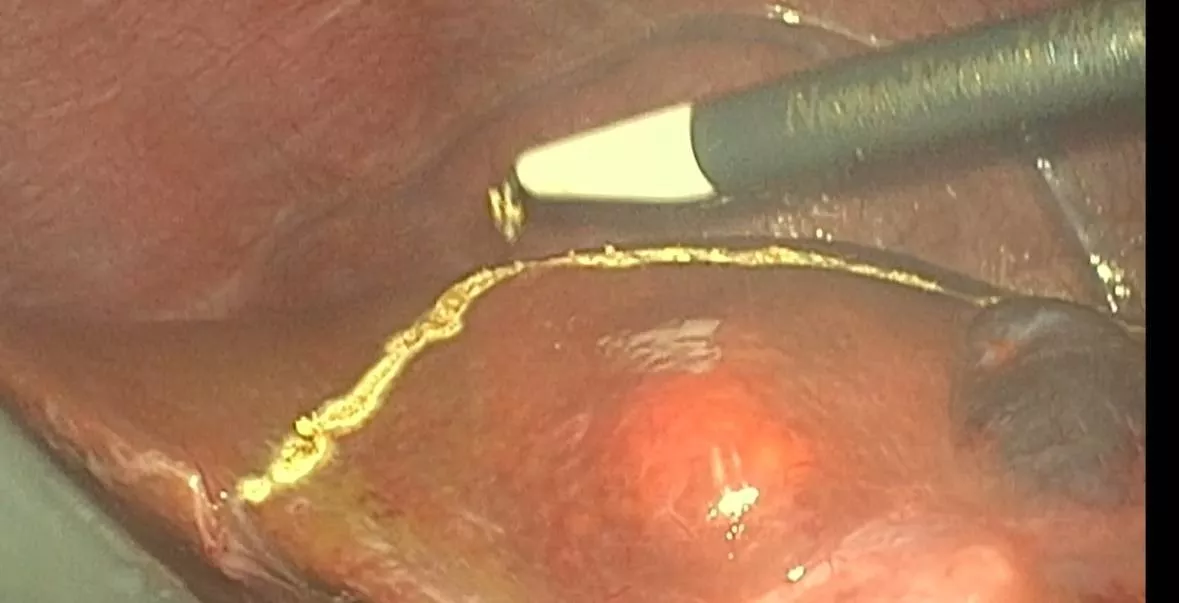
- Surgical Steps:
- Robotic port insertion and docking; subcutaneous flap dissection preserving nipple–areolar complex.
- En bloc excision of breast tissue and axillary dissection (levels I & II) with nerve preservation.
- DIEP flap harvested from lower abdomen, tunneled into mastectomy pocket, inset to reconstruct breast.
- Donor and recipient sites closed with drains.
- Intraoperative Findings: Fibrotic desmoplastic area in upper outer quadrant and retro-areolar region; few enlarged axillary nodes.
- Surgical Outcome: Complete oncologic resection with negative margins; flap inset with good vascularity.
Postoperative Course:
- Uneventful; flap healthy, no infection or necrosis.
- Discharged on POD-4 with standard postoperative care.
Final Histopathology:
- Specimen: Left nipple-sparing mastectomy with axillary dissection.
- Findings: No residual invasive carcinoma (ypT0), no DCIS; 16 axillary nodes negative (0/16); margins and nipple/subareolar tissue negative.
- Pathological Stage: ypT0N0 (AJCC 8th edition); Residual Cancer Burden 0 (complete pathological response).
Discussion:
Robotic-assisted R-NSSM allows precise dissection, minimal trauma, and superior cosmetic outcomes. DIEP flap reconstruction provides whole-breast coverage with excellent aesthetic results without compromising oncologic safety. Complete pathological response confirms efficacy of neoadjuvant chemoimmunotherapy and predicts favorable prognosis.
Conclusion:
Robotic nipple- and skin-sparing mastectomy with DIEP flap reconstruction is feasible, safe, and cosmetically excellent in selected TNBC patients achieving pathological complete response.